
You're tired, bloated, foggy, and not fully buying the easy explanations anymore. Maybe you've been told it's stress, “just IBS,” low iron, too much coffee, too little sleep, or that you should cut gluten and see what happens. That advice sounds practical, but it often creates a bigger problem. If celiac disease is a possibility, guessing first can make testing harder later.
That's where a celiac disease blood test becomes useful. It's the front door to the workup. Not the whole diagnosis, but the first meaningful signal. If you understand how that testing pathway works before you order anything or change your diet, you avoid the most common mistakes and make your next move far more efficient.
A lot of people in this situation are also trying to solve adjacent issues at the same time. Fatigue gets blamed on low iron. Bloating gets blamed on random food sensitivity. Brain fog gets brushed off because routine labs look “fine.” Sometimes checking related markers like ferritin for iron storage adds context, but if gluten is driving an autoimmune response, you need the right celiac labs and the right setup.
The Hidden Cause of Your Fatigue and Bloating
Some symptom patterns are noisy but not random.
You eat and feel distended. Your energy dips hard in the afternoon. You wake up tired, your focus is worse than it used to be, and your digestion seems unreliable in a way that's hard to pin to one meal. Then the self-experimenting begins. Remove bread. Add probiotics. Try digestive enzymes. Cut dairy. Reintroduce oats. Repeat.
That cycle wastes time because celiac disease doesn't behave like a simple food intolerance. It's an immune process. If gluten is the trigger, the body can produce antibodies that show up on the right blood tests. But that only helps if you test before you erase the signal.
Practical rule: If celiac disease is even a serious possibility, don't start a strict gluten-free diet before getting the proper blood work arranged.
The frustrating part is the usual pathway can feel like a black box. Book a primary care visit. Try to explain symptoms that come and go. Hope the right tests get ordered. Wait. Get a partial answer. Then maybe get referred again.
For a motivated patient, the better move is to understand the sequence. First, get the right serology. Then interpret it in context. Then decide whether you need gastroenterology follow-up and possible biopsy. That's a cleaner process than swinging blindly between elimination diets and internet theories.
Here's the angle that matters: a celiac disease blood test is most useful when you treat it like a tactical checkpoint, not a random lab order. Done correctly, it can move you from vague suspicion to a much sharper decision about what comes next.
Decoding the Celiac Serology Panel
A good celiac workup answers more than one question at once. Is the main antibody signal present? Can you trust an IgA-based result? Do you need a backup marker because age or immune status makes the standard screen less reliable?

Why the panel matters more than a single marker
Celiac serology works best as a small diagnostic toolkit, not a one-off lab add-on. If you order only one marker, you can miss the reason a result looks negative, borderline, or inconsistent with symptoms.
The anchor test is tTG-IgA. For patients age 2 and older, it is the standard first-line blood test in primary care and gastroenterology because it performs well as an initial screen, according to the AAFP review on celiac testing. If you are comparing direct-to-consumer or cash-pay options, a tissue transglutaminase antibody test panel is often the first useful search term. The practical catch is that the order only helps if you know what should sit beside it.
That is where patients get tripped up. A private lab order can be faster and sometimes cheaper than waiting for a clinic visit, but speed does not fix a poorly chosen panel. The point is not just to get blood drawn. The point is to get an answer you can act on.
What each test is doing
Here is the functional breakdown:
Test | Main job | Why it matters |
|---|---|---|
tTG-IgA | Primary screening marker | Best first signal in most people age 2 and older |
Total IgA | Checks overall IgA status | Helps catch IgA deficiency, which can make IgA-based celiac testing misleading |
DGP-IgA / DGP-IgG | Backup and special-case markers | More useful in younger children and in some situations where IgA-based testing is less dependable |
EMA-IgA | Confirmatory-style antibody marker | Often used as a higher-specificity follow-up test rather than the first screen |
Two pieces matter more than patients are usually told.
Total IgA is the quality check. If someone has IgA deficiency, a celiac panel built around IgA antibodies can look falsely reassuring. In practice, that means a negative tTG-IgA is not always the end of the story if total IgA is low.
DGP antibodies help cover the blind spots. The AAFP review notes that adding these markers is useful in younger children, where the standard adult-style approach is less dependable. That is one reason many clinicians order a panel instead of trying to outsmart the process with a single test.
EMA-IgA usually plays a supporting role. It is often treated as a stronger confirmation signal after a positive or suspicious first screen, rather than the first test to order on its own.
A practical way to read the panel is simple. tTG-IgA asks, “Is the usual celiac antibody signal present?” Total IgA asks, “Can I trust an IgA-based result?” DGP asks, “Do I need a backup route?” EMA asks, “How convincing is this positive pattern?”
If you remember one framework, use this one: start with the lead marker, verify that the immune background makes the result interpretable, and add the backup markers when the situation calls for them. That approach saves money, cuts repeat testing, and gives you a cleaner discussion with a GP or gastroenterologist if the next step becomes specialist follow-up.
How to Prepare for Your Celiac Test The Gluten Challenge
You clean up your diet because bread and pasta seem to wreck you. Two weeks later, you finally order the blood work. The result comes back negative, but the test was set up to miss the answer.
That sequence is common, and it creates a mess. You still have symptoms, but now you have a result that may not reflect what your immune system does when gluten is present.

Why diet changes can sabotage the test
Celiac serology works like a smoke alarm. It only goes off when there is enough smoke. If gluten has been removed, the antibody signal can fade, and the lab may report a negative or borderline result even though celiac disease is still on the table.
That is the practical rule to remember. If you want a celiac blood test to mean much, you need to be eating gluten before the draw.
This is also why timing matters more than many people realize. A rushed private lab order after a month of “mostly gluten-free” eating can waste money just as easily as a delayed NHS or primary care test. Cheap testing is only a good deal if the setup is right.
If you want to understand why many panels include a general immune check, review what serum IgA testing measures. It does not diagnose celiac disease on its own, but it helps show whether IgA-based celiac markers are interpretable.
What to do before the blood draw
Use a simple checklist.
Keep gluten in your diet. “Mostly gluten-free” is often enough to blur the result.
Be consistent. A single gluten-heavy meal right before testing does not recreate steady exposure.
Order the right tests before changing your diet. If celiac is a real possibility, get the blood work arranged first, then experiment later.
Plan follow-up before you test. If the result is positive or unclear, know whether your GP, a gastroenterologist, or a private specialist will handle the next step.
Here's a useful walkthrough on the broader issue of gluten challenge and why patients struggle with it:
The question people usually ask next is how much gluten they need and for how long. There is no smart reason to pretend one homemade protocol fits everyone. Symptom severity, how long you have been gluten-free, and how quickly you need an answer all change the plan.
My practical advice is simple. Do not guess if you have already been strictly gluten-free and get very symptomatic with reintroduction. That is the point where clinician input saves time, repeat testing, and a lot of avoidable confusion.
The requirement itself is straightforward: if you have already removed gluten completely, standard celiac blood testing becomes much less reliable.
Interpreting Your Celiac Blood Test Results
A common expectation is a yes-or-no answer from a celiac disease blood test. The better way to think about it is signal strength.
A weak or absent antibody signal means one thing. A strong, clear signal means another. The interpretation also depends on whether you were eating gluten at the time and whether the right companion tests were included.
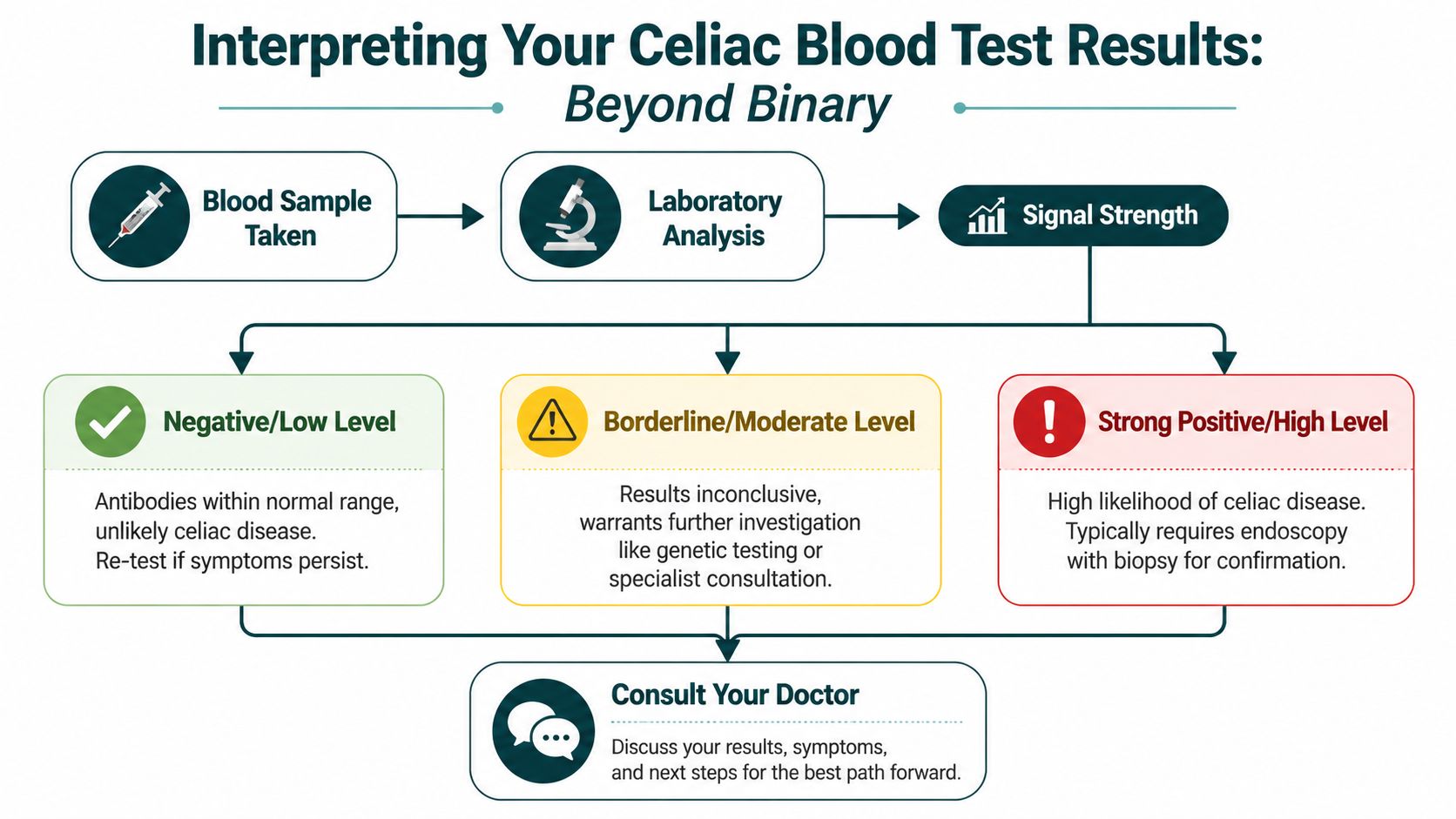
Think in terms of signal strength
A negative result is most useful when the setup was right. If you were actively eating gluten and the lab used the appropriate serology, a negative tTG-IgA is strong evidence against celiac disease. The AAFP review reported a negative predictive value of 99.0% for tTG-IgA in the right context, which is why it's such a valuable screening test in the first place, as summarized in the earlier AAFP reference.
Then there's the borderline zone. Here, people often get frustrated. Borderline or modest elevations don't settle the issue cleanly. They raise suspicion, but they don't finish the job. In practice, clinical context matters most in this situation. Symptoms, family history, total IgA status, and specialist follow-up start carrying more weight.
A strong positive result changes the conversation. The stronger the antibody elevation, the less likely it is to be random noise.
What a positive result does and does not mean
The most important nuance is this: positive serology is not the same thing as a final diagnosis.
Canadian guidance notes that a positive blood test should still lead to intestinal biopsy in most cases, and it also points out that home testing can't replace biopsy and that genetic testing is not diagnostic, according to the Canadian Celiac Association blood testing guidance. That same document highlights a practical source of confusion. A positive result can still be false positive.
Here's where the data gets especially interesting. In a large U.S. study discussed in that Canadian guidance, tTG-IgA levels above 10 times the upper limit of normal were highly specific for celiac disease. But that threshold applied to fewer than 10% of adults with biopsy-confirmed disease, and to only about 1% of patients seen at tertiary centers. In other words, a very high result can be highly informative, but most adults with celiac disease won't present with that dramatic pattern.
Clinical reality: A very high antibody level is a strong signal. It is not permission to skip context, and in most adults it still doesn't replace the full diagnostic conversation.
The same Canadian guidance notes an intestinal biopsy is still needed because of a 10% possibility of a falsely positive result. That's the part many simplified explainers skip. A positive blood test means “this needs confirmation and interpretation,” not “case closed.”
When a negative result is reassuring
A negative result is often where people underreact or overreact.
If you were eating gluten consistently, the right markers were ordered, and total IgA status was accounted for, a negative result is reassuring. It makes active celiac disease less likely. That doesn't mean your symptoms aren't real. It means you may need to look elsewhere. Another gastrointestinal condition, another food issue, another immune problem, or a non-GI contributor entirely.
If the result is negative but you had already reduced gluten, then the result has less value. That's not the lab failing. That's a setup problem.
A useful way to frame the result is this:
Negative with proper gluten intake: celiac disease becomes less likely
Positive: celiac disease becomes more likely, but still needs diagnostic confirmation
Borderline or confusing: this is the zone where specialist interpretation matters most
Advanced Testing and Common Diagnostic Pitfalls
You get a positive antibody result, cut gluten right away, feel a bit better, and assume the hard part is over. In practice, that is where the testing pathway often gets messy. The next move depends on why the result is unclear in the first place.

Where genetics fits
HLA genetic testing works best as a rule-out tool. A positive HLA-DQ2 or HLA-DQ8 result does not diagnose celiac disease, because a lot of people carry those genes and never develop the condition. A negative result is the part that carries more weight. If those risk genes are absent, celiac disease becomes much less likely.
That makes genetic testing useful in a narrow set of situations. Someone went gluten-free before proper blood work. A child or sibling of a person with celiac wants to understand long-term risk. A biopsy and serology do not line up cleanly. In those cases, genetics can help sort out the probability without pretending to answer the whole question.
If you are arranging testing yourself, this matters for cost control. Genetics is usually not the first thing to buy. Start with the markers that can detect active disease while you are still eating gluten. A full celiac panel option makes more sense than piecing together random tests one by one and then realizing a missing marker limited the result.
The pitfall many people miss
IgA deficiency is one of the easiest ways to misread celiac blood work.
Standard screening often relies on IgA-based antibodies, especially tTG-IgA. If total IgA is low, that result can look falsely reassuring. The lab did its job. The setup was incomplete. That is why experienced clinicians usually want total IgA checked alongside the main antibody test, then switch to IgG-based markers if IgA is low.
Use this logic:
Situation | What it means for testing |
|---|---|
Normal total IgA | IgA-based serology usually gives the clearest signal |
Low total IgA or confirmed IgA deficiency | IgG-based assays become more useful |
Already reduced or removed gluten | Antibody testing loses sensitivity |
Positive blood work with a confusing clinical picture | Gastroenterology follow-up, and often biopsy, still matters |
A second pitfall is timing. People often start a gluten-free diet before finishing the workup. I understand the impulse. If gluten seems to be wrecking your energy, gut, skin, or mood, waiting can feel irrational. But from a diagnostic standpoint, removing gluten too early can erase the signal you were trying to measure.
A third pitfall is overreading a weak positive result. Mild antibody elevations can happen in other autoimmune or inflammatory settings. That does not make the result meaningless. It means context matters more. Symptoms, gluten intake, total IgA status, repeat testing, and biopsy planning all become part of the decision.
This is also where system friction gets in the way. Delays between first suspicion, lab ordering, specialist review, and endoscopy often push people to self-experiment before the basics are complete. The broader problem is not unique to celiac testing. It is part of the larger issue of optimizing patient access in healthcare.
The practical goal is simple. Match the next test to the specific reason your result may be misleading, and do it before diet changes blur the picture.
How to Get Your Celiac Test Privately and Affordably
The old route is familiar. Book a visit, explain symptoms, wait for orders, wait for the draw, wait for review, then decide whether you need a referral. That path can work well, but it's not always fast, private, or easy to manage if you have a high-deductible plan or you just want to start with data.
Traditional route versus direct access
Direct-access testing appeals to people who want fewer gates between suspicion and useful information.
That doesn't replace clinical care. It shortens the distance to the first checkpoint. For something like celiac serology, that can be valuable because timing matters. If you're still eating gluten now, getting the right blood work arranged sooner is often better than waiting until you've changed your diet and blurred the signal.
There's also a broader systems issue here. A lot of healthcare friction happens before treatment ever starts. Scheduling, intake, handoffs, and delays are often the main bottleneck. If you're interested in the bigger picture, this overview of optimizing patient access in healthcare is a useful lens for understanding why even simple testing pathways can feel harder than they should.
If you want to order labs privately, one option is to use Goodlabs test booking. Goodlabs is a health platform that gives blood donors free clinical-grade lab panels (run at Quest or Labcorp), and offers the same panels at low cost to anyone who doesn't want to donate. That model is practical for people who want transparent access to testing without turning the process into a subscription or a long administrative project.
The true benefit isn't just convenience. It's clarity. A properly timed celiac disease blood test can turn a foggy symptom story into a much sharper conversation with your physician about what deserves confirmation, what doesn't, and what to investigate next.
FAQs Celiac Disease Blood Test 2026
Can you take a celiac disease blood test after going gluten-free?
Not reliably in many cases. Standard celiac antibody tests work best while you're actively eating gluten, because the immune signal can fall on a gluten-free diet.
What's the best first celiac disease blood test?
The usual first-line approach is tTG-IgA plus a total IgA level. That combination helps screen for celiac disease and checks whether IgA deficiency could distort the result.
Does a positive celiac blood test mean you definitely have celiac disease?
No. A positive result raises suspicion, but serology alone is not usually the final diagnosis. Many patients still need specialist follow-up and often intestinal biopsy.
What if my celiac blood test is negative but I still have symptoms?
A negative result lowers the odds of celiac disease if you were eating gluten and the right tests were used. If symptoms persist, another cause may need investigation.
Is genetic testing better than antibody testing for celiac disease?
Not for diagnosis. Genetic testing is mainly useful for ruling celiac disease out in certain situations. A positive genetic result shows risk, not confirmed disease.
If you want a simpler way to act while the signal is still clear, Goodlabs lets you book clinical-grade blood testing through CLIA-certified partner labs, with free panels available for qualifying blood donors and low-cost options for everyone else. That makes it easier to get useful data privately, while you're still eating gluten, and bring cleaner information into the next conversation with your physician.
Blood test results are informational and not a medical diagnosis. Talk to your physician about what your results mean for you.

Jake Kaiser
jakesjourney.co



