
Biomarker content often fails in the same way. It gives definitions, lists a few lab values, and leaves out the part that matters in real life: which tests change decisions before a problem becomes obvious.
A routine physical is designed to catch overt disease. It is not built to help an engaged adult track early movement in cardiovascular risk, blood sugar control, inflammation, nutrient status, or thyroid function. That gap matters, because many useful markers shift long before symptoms are clear or a standard panel raises concern.
A better approach is to treat biomarkers like a health dashboard, not a trivia list. Some markers are better for baseline risk. Others are better for monitoring response after you change diet, training, sleep, supplementation, or medication. That distinction explains why this guide focuses on a practical catalog of blood biomarkers: what each marker represents, where it fits clinically, which panels usually include it, who should consider testing, and what to do next if a result comes back out of range or off your usual pattern. For readers who want more context on heart-related testing, this guide to cardiac biomarkers and what they measure is a useful complement.
Goodlabs is a health platform that gives blood donors free clinical-grade lab panels, run at Quest or LabCorp, and offers the same panels at low cost to people who do not want to donate. That makes repeat testing more realistic, which is the main bottleneck for prevention. One isolated lab result can be interesting. A measured trend is what helps you act with confidence.
This guide stays focused on blood-based examples of biomarkers you can use. If fatigue or brain fog is part of the reason you are testing, it also helps to understand B12 D iron deficiency.
Table of Contents
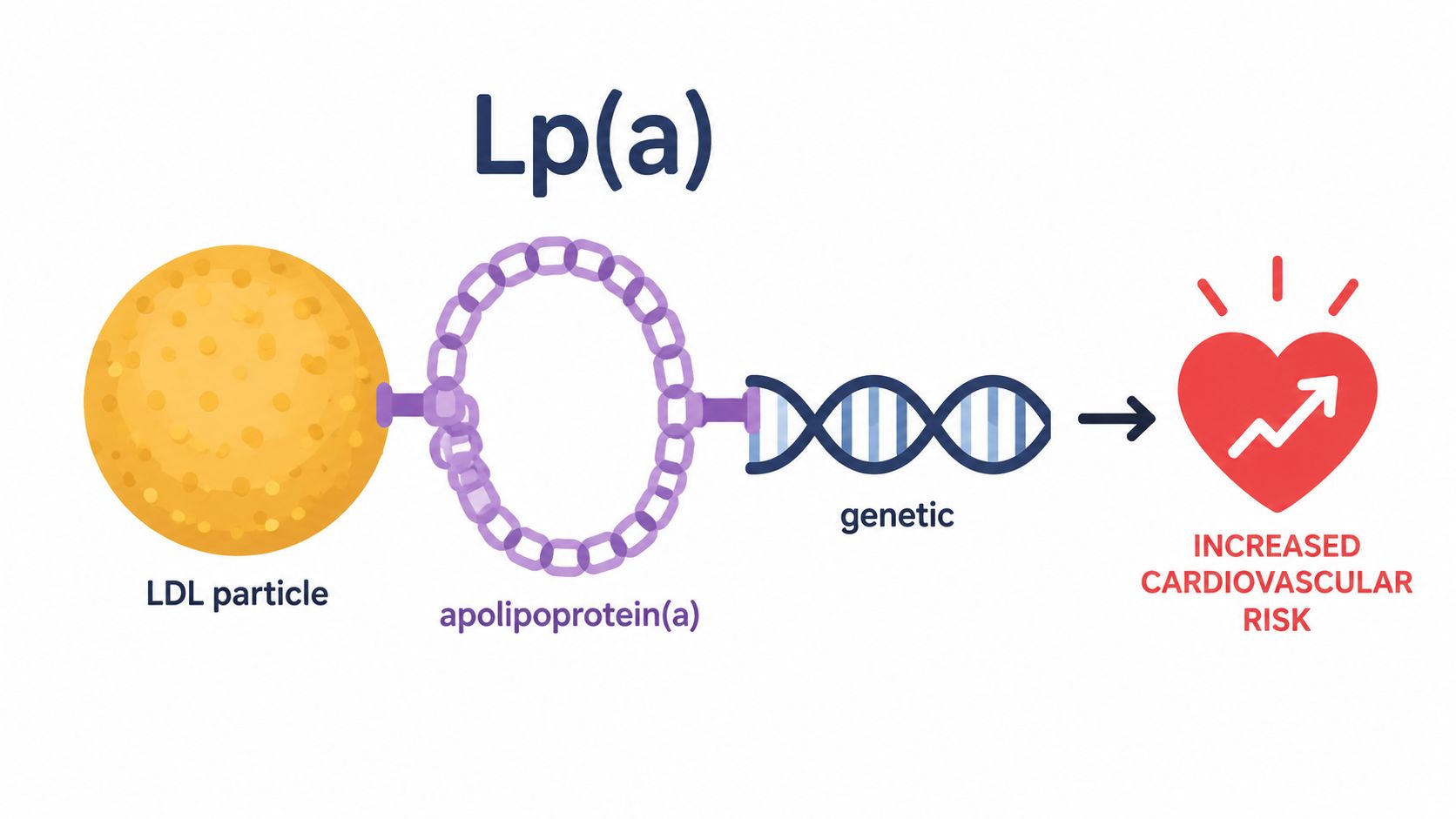
1. Lipoprotein(a) - Lp(a)
Lp(a) is one of the most practical examples of biomarkers because it answers a question a standard lipid panel often misses: are you carrying inherited cardiovascular risk that lifestyle alone may not fully explain? In practice, this is the marker I want people to know about early, especially if heart disease runs in the family.
It behaves differently from routine cholesterol markers. You can improve diet, training, sleep, and body composition, and still have high Lp(a) because much of the signal is inherited. That makes it less useful as a week-to-week scorecard and more useful as a baseline risk flag.
Why Lp(a) changes the conversation
If LDL is the traffic on the road, Lp(a) is a higher-risk vehicle type moving through the same system. You may not feel anything from it, but it can change how aggressively you and your physician think about overall prevention.
A practical way to use it:
Get a baseline early: This is especially useful if you have a family history of early cardiovascular events or unexplained “normal labs” in relatives who still developed disease.
Treat it as context, not panic: One result doesn't tell the whole story. It tells you whether the rest of your prevention plan should be tighter.
Use it with other cardiac markers: Pair it with broader cardiovascular testing, not in isolation. Goodlabs has a deeper explainer on cardiac biomarkers.
Practical rule: Lp(a) is most useful when it changes how seriously you take the rest of your risk profile.
What doesn't work is checking Lp(a) over and over like a lifestyle progress metric. Typically, it's a “know it, document it, and plan around it” biomarker.
2. Apolipoprotein B (ApoB)
ApoB is one of the most useful blood markers for people who want a sharper view of cardiovascular risk than LDL cholesterol alone provides. ApoB is the structural protein carried on atherogenic lipoprotein particles, so it gives you a better read on particle burden, not just how much cholesterol those particles are carrying.
That distinction matters because two people can have similar LDL cholesterol and very different particle-related risk. In real life, that discordance shows up a lot in people with insulin resistance, higher triglycerides, central adiposity, or mixed lipid patterns.
Why particle count beats simple cholesterol watching
Think of LDL cholesterol as the amount of cargo and ApoB as the number of trucks on the highway. Damage risk often tracks better with the number of particles colliding with artery walls than with the total cargo weight.
This is why ApoB has become part of many prevention-focused conversations. It's not replacing every older marker, but it often clarifies who needs a more serious plan and who may be overestimating safety based on a “fine” standard lipid panel.
A practical approach:
Order it with a standard lipid panel: ApoB is strongest when you compare it with LDL-C, HDL, and triglycerides.
Watch trends after changes: If you're changing diet, training, weight, or medications, ApoB is often a better scorecard than LDL alone.
Pay attention in metabolic dysfunction: This marker earns its keep when the usual cholesterol story looks cleaner than the underlying risk likely is.
What doesn't work is treating ApoB like a standalone verdict. It's a better lens, not the whole picture.
3. High-Sensitivity C-Reactive Protein (hs-CRP)
hs-CRP gets treated like a verdict far too often. In practice, it works better as a smoke alarm. It can flag low-grade inflammation linked with cardiometabolic risk, but it does not tell you where the fire is.
That distinction matters because hs-CRP rises for many reasons. A cold, hard training block, poor sleep, gum inflammation, an injury, or extra visceral fat can all push it up. If you want this marker to be useful, test it under stable conditions and read it as part of a larger pattern.
How to use it without getting fooled by noise
The best time to measure hs-CRP is when life is boring. No active infection. No recent race or unusually hard lifting cycle. No obvious recovery debt. Otherwise, you may be measuring a short-term flare instead of your usual inflammatory baseline.
I treat hs-CRP as a context marker, not a standalone score. A higher result means the next step is to look for plausible drivers: waist size, sleep quality, alcohol intake, oral health, training load, recent illness, and markers tied to cardiometabolic risk. If that broader pattern points toward insulin resistance or excess central adiposity, this guide to metabolic health markers and risk patterns is a useful next read.
A practical framework:
Test at baseline: Wait until you are past acute illness, injury, or unusually heavy exertion.
Pair it with related data: Lipids, blood pressure, glucose markers, body composition, and symptoms make hs-CRP more interpretable.
Repeat before reacting: One unusually high result can be random. A persistent pattern deserves follow-up.
Look for causes you can fix: Weight loss, better sleep, treating dental issues, improving food quality, and reducing excess alcohol often matter more than chasing the number itself.
Goodlabs covers the wider use case in its guide to inflammation markers blood test options.
4. Hemoglobin A1C (HbA1c)
HbA1c gets treated like a diabetes marker. That is too narrow.
In practice, it is one of the clearest blood markers for seeing whether your glucose control has been subtly improving, drifting, or sliding for a while. Unlike a single fasting glucose reading, HbA1c captures the broader pattern. That makes it useful for diagnosis, useful for follow-up, and useful for people who want a better read on metabolic health before obvious problems show up.
Why HbA1c earns a spot on almost any health dashboard
Fasting glucose works like one photo. HbA1c works like the highlight reel from the past few months.
That trade-off matters. HbA1c is better for trend detection, but it can miss short-term glucose volatility. Someone can post a "fine" HbA1c and still have large post-meal spikes, especially if sleep is poor, activity is low, or meal composition is inconsistent. On the other side, one fasting glucose result can look off after a bad night of sleep, stress, or a tough training block. HbA1c helps smooth some of that noise.
This marker belongs in a practical catalogue of biomarkers because it answers several useful questions at once. Is glucose control stable? Is a lifestyle change large enough to show up in blood work? Should you stop relying on guesswork and test more thoroughly?
Who should pay attention here? Adults with a family history of diabetes, rising waist size, low activity, high stress, poor sleep, polycystic ovary syndrome, or a long stretch of convenience-food eating. It is also a smart baseline test for people who feel "mostly okay" but know their habits have slipped.
A simple framework:
Use HbA1c as a baseline: It is one of the easiest ways to establish whether your current routine is working.
Retest after a real intervention: Fat loss, resistance training, walking after meals, higher protein intake, and better sleep are easier to judge when you compare results over time.
Pair it with other glucose data: Fasting glucose, fasting insulin, or even home glucose monitoring can reveal patterns HbA1c alone may miss.
Interpret it in context: Symptoms, body composition, medications, and overall risk pattern still matter.
For readers trying to place glucose markers inside a broader lab strategy, Goodlabs explains how related tests fit together in its guide to interpreting hormone panel results and connected blood markers.
5. Thyroid-Stimulating Hormone (TSH) and Free T4
Plenty of people say they “tested thyroid” when what they really mean is they checked TSH once. That's often too shallow. TSH is a control signal from the pituitary. Free T4 is one of the main circulating thyroid hormones. Looking at both gives you a more useful read on the axis.
This is one of the best examples of biomarkers where pairing matters more than any single result. Fatigue, cold intolerance, mood changes, constipation, hair changes, and unexplained weight shifts all push this pair higher on the list.
Read the thyroid axis, not a single number
Think of TSH as the thermostat signal and Free T4 as the heat coming out of the system. If you only measure one, you can miss the pattern.
Real-world testing often breaks down. A person gets a “normal” TSH, keeps feeling off, and stops asking questions. Sometimes that's appropriate. Sometimes it means the workup was incomplete.
A practical use case:
Start with both markers: TSH alone can leave important gaps.
Retest when symptoms persist: Especially if sleep, stress, calorie intake, and training load don't explain how you feel.
Escalate thoughtfully: If the pattern suggests thyroid dysfunction, additional antibody testing may become useful through your physician.
For people trying to make sense of hormone-related blood work more broadly, Goodlabs has a primer on hormone panel results.
6. Vitamin D (25-Hydroxyvitamin D)
Vitamin D sits in an odd spot. It's popular, often tested, and often oversimplified. The right marker is 25-hydroxyvitamin D, because that's the main circulating form used to assess overall vitamin D status.
This is one of the biomarkers where context changes everything. Sun exposure, season, latitude, skin tone, diet, supplementation habits, and absorption issues can all shape the result.
A useful marker with a lot of context
Vitamin D is best treated as a maintenance biomarker, not an abstract wellness badge. If you spend most of your day indoors, train early or late, use sun protection consistently, or live in a place with long low-sun stretches, your result may drift even if your routine feels healthy.
What works:
Test seasonally if your exposure changes a lot: Winter and summer can tell very different stories.
Recheck after starting supplementation: A number only becomes useful when you confirm whether your plan changed it.
Look at symptoms and lifestyle too: Low energy, bone-health concerns, and low sunlight exposure make the result more actionable.
What doesn't work is megadosing blindly because you assume more is better. This marker is most helpful when it guides a targeted, measured response.
7. Iron Panel (Serum Iron, Ferritin, TIBC, Transferrin Saturation)
Iron status is where a lot of self-directed testing goes wrong. People test ferritin alone, see one number, and build a whole narrative around it. That's risky. Iron biology is more dynamic than that, which is why a proper panel usually works better.
A full iron panel gives you different angles: circulating iron, stored iron, transport capacity, and how saturated the transport system is. That combination helps sort out whether low energy is more likely tied to iron stores, transport, inflammation, or something else.
Why ferritin alone can mislead you
Ferritin is useful, but it can rise in inflammatory states. That means an apparently reassuring ferritin result doesn't always mean iron status is fine. This is one of those places where panel thinking beats single-marker thinking every time.
If you donate blood regularly, train hard, menstruate, eat little red meat, or have unexplained fatigue, iron testing becomes more practical. It's also one of the most common areas where symptoms are blamed on stress when there may be a nutritional or donation-related contribution.
A quick rule set:
Use a full panel for fatigue: Don't anchor on serum iron or ferritin alone.
Pair it with a CBC when needed: That helps separate iron issues from other anemia patterns.
Interpret ferritin carefully when inflammation is present: Context matters.
If you want a plain-English walkthrough of deficiency patterns, this short video is useful:
8. B12 and Folate (Cobalamin and 5-Methyltetrahydrofolate)
B12 and folate are easy to underestimate because deficiency can look vague at first. Low energy, brain fog, numbness, mood changes, and abnormal blood counts can all overlap with dozens of other problems. That's exactly why these markers belong on a practical list.
These are also good examples of biomarkers where lifestyle pattern matters a lot. Vegan and vegetarian eating patterns, low animal-food intake, absorption issues, some medications, and increased physiological demands can all shift the picture.
When these markers deserve extra attention
B12 and folate support red blood cell production and neurologic function. If either is off, the body often sends mixed signals rather than one obvious symptom cluster.
A good biomarker only helps when you connect it to a decision. For B12 and folate, that usually means asking whether diet, absorption, medications, or higher demand is the most likely driver.
Practical use beats generic advice:
Check them in fatigue or neuropathy workups: Especially when symptoms persist despite decent sleep and training habits.
Pay closer attention if you avoid animal foods: B12 status can drift gradually.
Use follow-up testing when the result is borderline: Borderline values plus symptoms often deserve a deeper look.
Goodlabs also has a broader resource on nutrient deficiencies if you're trying to connect low-energy symptoms to a fuller nutrition picture.
9. Homocysteine
Homocysteine isn't a first-line marker for everyone, but it can be a smart second-layer test. It sits at the intersection of methylation, B-vitamin status, and cardiovascular and neurologic risk interpretation, which is why prevention-focused clinicians often use it when the basic panel leaves unanswered questions.
The best use case isn't random curiosity. It's targeted clarification. If someone has a strong family history of early cardiovascular disease, unexplained vascular risk, or borderline B12 and folate patterns, homocysteine can add signal.
Best use case for homocysteine
I think of homocysteine as a systems marker. It doesn't point to one issue cleanly, but it can tell you that the one-carbon metabolism machinery may deserve more attention.
That means it works best in combinations:
With B12 and folate: It can help interpret whether borderline vitamin status may be functionally meaningful.
With cardiovascular context: Family history and other lipid markers make it more relevant.
With retesting after intervention: If supplementation or dietary changes are used, a repeat result can show whether the plan moved the biology.
What doesn't work is treating high homocysteine as a diagnosis by itself. It's a clue, not a conclusion.
10. Magnesium
Magnesium is one of the most commonly discussed nutrients and one of the most poorly interpreted lab markers. People hear that magnesium matters for sleep, muscle function, nerve signaling, blood pressure, and glucose control, then assume one serum result settles the issue. Usually it doesn't.
This is one of the better examples of biomarkers for understanding a trade-off between convenience and depth. Serum magnesium is easy and common. It's also not always the best reflection of total-body status in people with suggestive symptoms.
A marker people often test too simplistically
If you have muscle cramps, headaches, palpitations, poor sleep, or high stress load, magnesium often enters the conversation. That doesn't mean supplementation should be automatic. It means the marker should be interpreted with symptoms, diet, GI health, medication use, and training load in mind.
A practical workflow looks like this:
Start with serum magnesium: It's accessible and still useful as a first pass.
Go deeper if symptoms persist: Red blood cell magnesium may offer more context in some cases.
Match the supplement form to the goal: People often tolerate and use different forms differently, so random buying isn't a strong strategy.
Don't chase magnesium because it's trendy. Chase it because the symptom pattern and lab context make it worth solving.
Quick Comparison of 10 Clinical Biomarkers
Biomarker | Implementation complexity 🔄 | Resource requirements ⚡ | Expected outcomes ⭐📊 | Ideal use cases 💡 | Key advantages |
|---|---|---|---|---|---|
Lipoprotein(a) - Lp(a) | Low-to-moderate 🔄: single blood test, needs specialist interpretation | Low ⚡: one assay, increasingly available; insurance variable | High ⭐📊: identifies lifelong inherited ASCVD risk, strong stratifier | Family history of early CVD; unexplained premature CAD; baseline CV risk | Detects genetic risk; one-time lifetime measure; enables family screening |
Apolipoprotein B (ApoB) | Low 🔄: single assay added to lipid panel | Low-to-moderate ⚡: routine lab, slightly higher cost than basic panel | High ⭐📊: superior particle-based risk prediction; guides therapy intensity | Metabolic syndrome, diabetes, discordant LDL vs risk; treatment titration | More accurate than LDL-C; identifies particle discordance; informs statin decisions |
High-Sensitivity C-Reactive Protein (hs-CRP) | Low 🔄: simple test but timing matters (avoid acute illness) | Low ⚡: inexpensive, widely available | Moderate ⭐📊: indicates systemic inflammation; non-specific risk marker | Inflammation assessment, borderline CV risk, monitoring anti-inflammatory therapy | Inexpensive; independent predictor; useful for treatment response tracking |
Hemoglobin A1C (HbA1c) | Low 🔄: standardized, routine lab test | Low ⚡: widely available, low cost | High ⭐📊: diagnoses/monitors diabetes; predicts micro/macrovascular risk | Diabetes screening/management; metabolic health surveillance | Gold standard for long-term glycemic control; single test reflects months |
TSH and Free T4 | Low-to-moderate 🔄: two tests required; clinical-context interpretation | Low ⚡: routine endocrine assays | High ⭐📊: detects hypo/hyperthyroidism; guides treatment for symptomatic relief | Fatigue, weight change, mood changes; routine screening ≥35 or symptomatic | Essential for thyroid diagnosis and medication monitoring; improves QoL when treated |
Vitamin D (25-OH) | Low 🔄: single assay; seasonal factors affect timing | Low ⚡: inexpensive; may require seasonal retesting | Moderate ⭐📊: identifies deficiency; correctable with supplementation | Limited sun exposure, athletes, northern latitudes, immune concerns | Easily correctable deficiency; impacts bone and immune health |
Iron Panel (Iron, Ferritin, TIBC, TSAT) | Moderate 🔄: multi-marker interpretation; inflammation confounds results | Moderate ⚡: multiple assays, possible repeat testing | High ⭐📊: diagnoses deficiency or overload; directs supplementation/transfusion | Fatigue/anemia workup, blood donors, athletes, suspected overload | Comprehensive iron status assessment; critical for donor safety and anemia management |
B12 and Folate | Low-to-moderate 🔄: straightforward assays; may need MMA/homocysteine for clarity | Low ⚡: widely available; add-on metabolites increase cost | Moderate ⭐📊: detects deficiencies that cause hematologic/neurologic issues | Vegans/vegetarians, preconception, macrocytic anemia, neuropathy | Correctable with supplementation; crucial in pregnancy and neurology |
Homocysteine | Moderate 🔄: single assay but requires nutritional/genetic interpretation | Moderate ⚡: specialized testing and follow-up (B‑vitamin assays/genetics) | Moderate ⭐📊: flags modifiable CV and cognitive risk; clinical impact debated | Early CVD family history, unexplained stroke, suspected B‑vitamin deficiency | Modifiable marker linking nutrition to CV/cognitive risk; trackable with supplementation |
Magnesium | Moderate 🔄: serum test simple but poorly reflects total status; RBC testing more complex | Moderate ⚡: serum common; RBC magnesium less available and costlier | Low-to-moderate ⭐📊: screens deficiency but limited sensitivity | Hypertension, cramps, arrhythmias, athletes with heavy sweat | Addresses common deficiency; informs supplementation impacting CV and neuromuscular health |
From Data to Action Build Your Health Dashboard
A long list of biomarkers does not give you a health strategy. A dashboard does.
The practical mistake I see is treating every lab value as equal. They are not. Some markers are best for one-time risk sorting, some are built for trend tracking, and some only make sense when you read them beside symptoms, training load, medications, sleep, and diet. The NIH NCATS biomarker development resource makes that distinction clearly. A biomarker is an objective measure, but its value depends on what decision you are trying to make.
That is the frame to use with this catalogue. Lp(a) is usually a one-time inherited risk marker. ApoB and HbA1c are better trend markers because repeat testing can show whether your plan is working. hs-CRP, ferritin, homocysteine, and magnesium are context-heavy markers. They work less like a scoreboard and more like warning lights on a car dashboard. A warning light matters, but you still need to check the engine.
Good dashboards also need clean lab identification. If you compare results across platforms, panel names can be messy and test labels can differ by lab. Matching the right assay matters, especially if you are tracking over time or importing data into an app. The LOINC code lookup API guide is useful for understanding how standardized lab codes help keep those comparisons accurate.
My rule is simple. Start with markers that change behavior, treatment intensity, or follow-up timing.
If a result will not alter what you do next, it probably does not belong in your first round of testing.
That is why this article goes beyond definitions. The useful question is not, “What is a biomarker?” The useful question is, “Which marker belongs on my dashboard, which panel includes it, how often should I repeat it, and what action would a high or low result trigger?” That approach keeps you from overspending on broad testing without a plan, while still catching the markers that can materially change prevention work.
Cancer care shows the same principle. PSA and CA-125 are used because they can affect follow-up and treatment decisions in the right clinical setting. HER2 matters because it identifies patients who may benefit from trastuzumab, as noted in this overview of biomarker analysis in precision medicine. The lesson carries over to consumer lab testing. A biomarker earns its place when it changes the next move.
Goodlabs is one route for putting that system into practice. It offers clinical-grade lab panels through participating blood centers for eligible donors, and the same tests can also be purchased directly. Value is not getting a pile of numbers. It is building a repeatable record of cardiovascular, metabolic, inflammation, nutrient, and hormone markers, then using those trends to ask sharper questions with your physician.
Blood test results are informational and not a medical diagnosis. Talk to your physician about what your results mean for you.
Goodlabs makes it easier to act on the biomarkers that matter. You can get clinical-grade testing free with an eligible blood donation or order panels directly without a subscription. Explore Goodlabs if you want a simpler way to track cardiovascular, metabolic, inflammation, nutrient, and hormone markers over time.

Jake Kaiser
jakesjourney.co



