Your Heart's True Risk: The Cardiovascular Markers You Need to Know
For decades, the conversation around heart health has been dominated by two simple terms: "good cholesterol" (HDL) and "bad cholesterol" (LDL). While this was a useful starting point, it is an outdated and incomplete picture. The science has evolved, and if we’re serious about understanding our risk for atherosclerotic cardiovascular disease (ASCVD), the leading cause of death worldwide [8], we need to upgrade our vocabulary.
ASCVD is the process where plaque that is made of fats, cholesterol, and other substances builds up inside your arteries. This buildup, known as atherosclerosis, hardens and narrows the arteries, eventually leading to heart attacks and strokes. It's a silent process that can begin decades before any symptoms appear.
Fortunately, modern blood tests can give us a highly accurate look at the root cause of this process. Forget the simplistic "good" vs. "bad" cholesterol model. It’s time to focus on the numbers that are causally linked to disease.
The New Gold Standard: Why ApoB is King
If you only track one number for your heart disease risk, this is it.
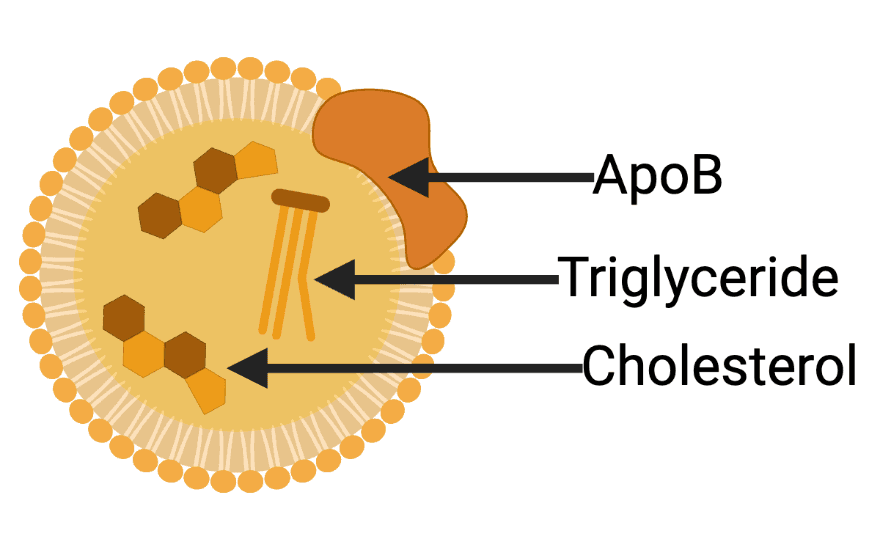
Apolipoprotein B (ApoB) is a protein that acts as the structural shell for every single lipoprotein particle that can penetrate the artery wall and cause plaque. This includes LDL, VLDL, and IDL particles. Think of ApoB as the captain of a ship. Every cargo ship navigating your bloodstream has exactly one captain. It doesn't matter if the ship is fully loaded with cargo (cholesterol) or sailing half-empty; it still requires one captain. Therefore, counting the captains tells you exactly how many ships are in the fleet, which is a far more accurate measure of traffic than just weighing the cargo [1].
Therefore, measuring your ApoB level is a direct count of the total number of atherogenic (plaque-causing) particles in your bloodstream.
Why it's better than LDL-C: Standard LDL-C (Low-Density Lipoprotein Cholesterol) tests measure the amount (mass) of cholesterol inside your LDL particles, not the number of particles. This is a critical distinction. You could have a "normal" LDL-C level but a very high number of small, dense LDL particles, putting you at high risk. ApoB clears up this confusion by simply counting every single threatening particle. It is a measure of quantity, not just volume [2].
Optimal: < 80 mg/dL
Acceptable: 80–100 mg/dL
High Risk: > 100 mg/dL
Very High Risk: > 120 mg/dL
The Genetic Wild Card: Lipoprotein(a) or Lp(a)
Lipoprotein(a), or Lp(a), is a specific type of LDL-like particle that is particularly aggressive in promoting both atherosclerosis and blood clots. What makes Lp(a) unique, and crucial to test, is that its level is almost entirely determined by your genes. Diet, exercise, and lifestyle have very little effect on it [3].
Why it matters: You can have perfect ApoB, low LDL-C, and a healthy lifestyle, but a high Lp(a) level can still confer a significant, independent risk for heart attack and stroke. Because it's genetic, you only need to test it once or twice in your life to know your baseline. A high level doesn't mean you are doomed; it means you and your doctor need to be much more aggressive in lowering your other risk factors (like ApoB) to offset the genetic handicap.
Low Risk: < 30 mg/dL
High Risk: > 30 mg/dL
Very High Risk: > 50 mg/dL
The Classic Markers (Viewed Through a Modern Lens)
While ApoB is the best single measure, the standard lipid panel still provides valuable context, especially since it's the test most people have access to. Here is how to interpret the old players in this new framework.
LDL Cholesterol (LDL-C): The Classic 'Bad Guy'
This is the marker everyone knows. For years, LDL-C was the primary target of therapy for preventing heart disease. It's certainly better than nothing, but it is crucial to understand what it's actually measuring.
What it is: LDL-C measures the total mass of cholesterol being carried within all your LDL particles. It does not tell you the number of LDL particles, which is the more important driver of risk. Imagine two scenarios: you could have a few large, fluffy LDL particles carrying a lot of cholesterol, or you could have a huge number of small, dense LDL particles carrying the same total amount of cholesterol. The second scenario is far more dangerous because you have more particles available to penetrate the artery wall [4]. LDL-C can't distinguish between these two states, whereas ApoB can.
The bottom line: A low LDL-C is good, but it's an imperfect proxy for risk. If your LDL-C is high, your ApoB is almost certainly high. But if your LDL-C is "normal," your ApoB could still be dangerously elevated.
Optimal: < 100 mg/dL (or < 70 mg/dL for those with heart disease or increased risk)
Borderline High: 130–159 mg/dL
High: ≥ 160 mg/dL
Triglycerides
These are fats circulating in your blood for your cells to use as energy. While necessary, high levels are a problem.
What they indicate: High triglycerides are often a sign of poor metabolic health and insulin resistance. They reflect how well your body is processing carbohydrates and fats. When TGs are high, it often means your liver is working overtime, packaging excess energy into atherogenic VLDL particles [5].
Optimal: < 100 mg/dL
Borderline High: 150–199 mg/dL
High: ≥ 200 mg/dL
HDL Cholesterol (HDL-C)
Known as "good cholesterol," HDL particles perform a process called reverse cholesterol transport, removing cholesterol from the artery wall and taking it back to the liver.
A nuanced view: While a higher HDL is generally better, we now know that the function of your HDL is more important than the absolute number. Very low HDL-C is a strong risk factor, often linked to insulin resistance. However, trying to artificially raise HDL with drugs has not proven to reduce cardiac events [6]. It is best viewed as an indicator of your overall metabolic health rather than a direct target for treatment.
Low (High Risk): < 40 mg/dL
Optimal: > 60 mg/dL
Triglyceride : HDL Ratio
This simple calculation is one of the most powerful proxies for insulin resistance and cardiovascular risk available on a standard lipid panel.
What it means: This ratio gives you a snapshot of the balance between the triglyceride-rich particles being produced by your liver and the "cleanup" crew of HDL particles. A high ratio strongly suggests insulin resistance and a bloodstream full of small, dense, and dangerous atherogenic particles [7].
Optimal: < 1.0
Good: < 2.0
High Risk: > 3.0
Your Action Plan: Knowledge is Power
Cardiovascular disease doesn't happen overnight. It's a slow burn that develops over a lifetime, driven directly by the concentration of atherogenic particles in your bloodstream.
Don't wait for symptoms. The first symptom of heart disease is too often a fatal heart attack. Be proactive. The next time you see your doctor, review your standard lipid panel with this new understanding. And if you're serious about knowing your true risk, ask for an ApoB test and an Lp(a) test.
Understanding these numbers gives you the power to intervene, letting you and your doctor create a precise, personalized strategy to lower your risk and protect your heart for the long haul.
Sources
[1] https://academic.oup.com/eurheartj/article/38/32/2459/3745109
[2] https://jamanetwork.com/journals/jamacardiology/article-abstract/2753612
[3] https://www.jacc.org/doi/full/10.1016/j.jacc.2016.11.042
[4] https://www.google.com/search?q=https://www.lipidjournal.com/article/S1933-2874(07)00104-4/fulltext
[5] https://www.ahajournals.org/doi/10.1161/CIR.0b013e3182160726
[6] https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60312-2/fulltext
[7] https://www.ahajournals.org/doi/10.1161/01.CIR.96.8.2520
[8] https://pmc.ncbi.nlm.nih.gov/articles/PMC8588746/

Jake Kaiser
jakesjourney.co